Pediatric Emergency Playbook
Tim Horeczko, MD, MSCR, FACEP, FAAP
All episodes
Best episodes
Top 10 Pediatric Emergency Playbook Episodes
Goodpods has curated a list of the 10 best Pediatric Emergency Playbook episodes, ranked by the number of listens and likes each episode have garnered from our listeners. If you are listening to Pediatric Emergency Playbook for the first time, there's no better place to start than with one of these standout episodes. If you are a fan of the show, vote for your favorite Pediatric Emergency Playbook episode by adding your comments to the episode page.
GI Bleeding in Children
Pediatric Emergency Playbook
10/01/16 • 33 min
The differential diagnosis of GI bleeding in children is broad.
(Here is the complete differential diagnosis)
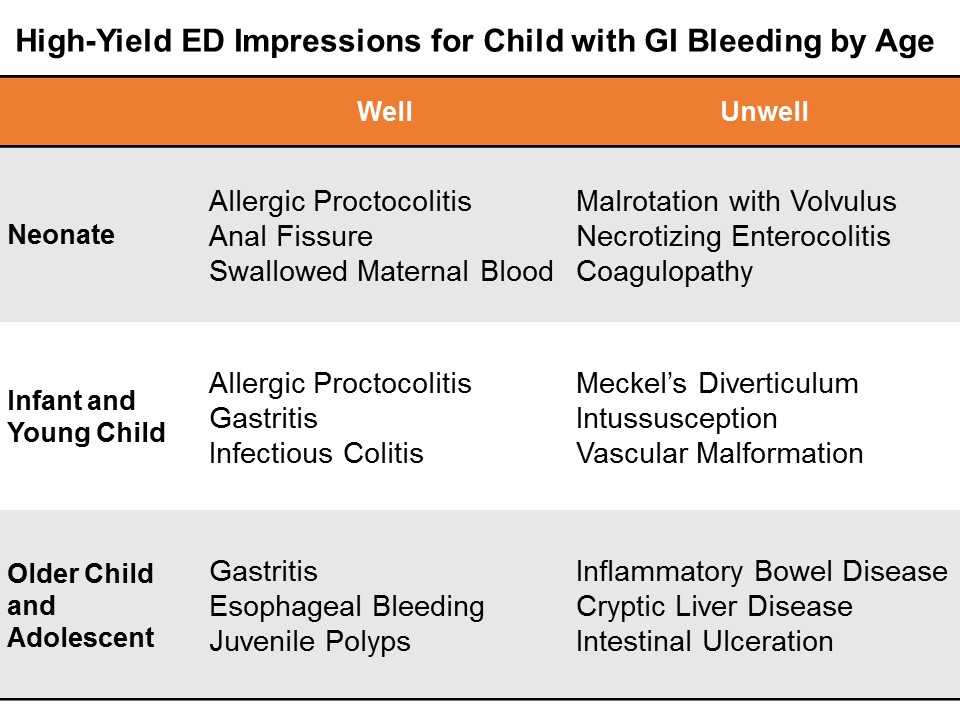
In the ED, we can simplify by categorizing by age and appearance. NeonatesGI bleeding in the neonate (less than one month of age) is serious until proven otherwise.
Well appearing?If this in obvious anal fissure, then no further work-up is necessary. Counsel on proper feeding and follow-up.
Evaluate for potential swallowed maternal blood by examining mother with a chaperone, then perform the Apt test.
Consider allergic proctocolitis if the child is well. Counsel the breastfeeding mother on diet modification. If formula fed, the child should feed through thus until the primary care physician decides whether to start the sticky process of changing up formulas.
If unclear, consider a complete blood count and/or further work-up and admission if unwell.
Ill Appearing?The three most dangerous diagnoses in the neonate are necrotizing enterocolitis, malrotation with volvulus, and inherited coagulopathy. It is important to note that 15% of necrotizing enterocolitis occurs in full-term babies; malrotation can present simply in shock, without initial overt bleed. Inherited conditions may not be known to the family early on, as they have not yet heard back from the neonatal screening done at birth.
Pitfalls in the neonate and infantGenitourinary bleeding; hematuria; or uric acid crystals: the classic fake out here is the orange or pink stained diaper – that is actually residue from deposits of uric acid crystals in the urine, an almost always benign phenomenon in which the concentrated crystals oxidize and stain the diaper, frightening the parents.
Think -- pink stain, without clot:
Infants and Young Children Well appearing?Through the first year to age 5, things like infectious colitis and gastritis are common.
Ill appearing?Think about intussusception, cryptic liver disease, or esophageal bleeding. Check the skin – is that a dark purple palpable rash on the buttocks? Think Henoch-Schoenlein purpura.
Focus: Meckel's DiverticulumMeckel’s diverticulum is the most common congenital malformation of the GI tract, and the most common cause of GI bleeding in the toddler. It is a remnant of the omphalomesenteric tract – it came from a long tube that once connected the yolk sac to the lumen of the midgut. A stranded island of gastric tissue secretes acid in the intestine, where it doesn’t belong. Sometimes these islands never cause much trouble.
When it does present itself, a Meckel’s diverticulum usually follows the rule of twos:
Presents by age 2 Affects 2% of the population Often 2 inches in length May include 2 types of mucosa Found within 2 feet of the ileocecal valve.
Not actively bleeding: technetium-99 pertechnate scintigram (Meckel’s scan).
Actively bleeding: radio-labeled red blood-cell scan (resuscitate and call your surgeons!)
Pitfalls in the infant and young childEpistaxis; food-related misadventures
Older Child and Adolescent Well appearing?Mallory-Weiss tears after forceful vomiting; trivial hemoptysis after viral symptoms; pill esophagitis in the child is just learning to swallow medications. Always consider foreign body ingestion.
Ill Appearing?Varices from cryptic liver disease; hemorrhagic gastritis; vascular malformation, such as a Dieulafoy lesion, where a tortuous small artery ends just superficial to the gastric mucosa, and can erode through and erupt.
Focus: Inflammatory Bowel DiseaseApproximately a quarter of patients with inflammatory bowel disease (IBD) -- both Ulcerative Colitis and Crohn disease – will present by age 20. Children and adolescents may present with the classic symptoms of IBD: abdominal pain, weight loss, bloody diarrhea, but many present atypically with isolated signs like poor growth, anemia, or delayed puberty.
You may also suspect IBD in the child with other extra-intestinal symptoms like oral ulcers, clubbing, erythema nodosum, jaundice, or hepatomegaly.
On history and physical examination, you may get one of three cardinal presentations
Fatigue, history of anemia, in a stable child who comes to the ED with bloody diarrhea
Chronic diarrhea, chronic abdominal pain, and poor weight gain or weight loss
A fulminant presentation, with ...
Multisystem Trauma in Children, Part Two: Massive Transfusion, Trauma Imaging, and Resuscitative Pearls
Pediatric Emergency Playbook
03/01/16 • 37 min
On arrival, he was in compensated shock, with tachycardia.
He decompensates and needs blood.
How do we manage his hemodynamics and when do we perform massive transfusion? Pediatric Massive Transfusion40 mL/kg of blood products given at any time within the first 24 hours.
Adolescents and Adult Massive Transfusion6-8 units of packed red blood cells (PRBCs)
- Adults have about 5 L of circulating blood.
- Not including plasma, one could replace all circulating erythrocytes with about 10 units of PRBCS
- The best ratio of PRBCs:Plasma:Platelets is unknown, but consensus is 1:1:1.
- 1 unit of PRBCS is typically 300 mL of volume.
The typical initial transfusion of PRBCs in children is 10 mL/kg.
Massive transfusion in children is defined as 40 mL/kg of any blood product.
Once you start to give a child with major trauma the second 10 mL/kg dose of PRBCs – start thinking about other blood components, and ask yourself whether you should initiate your massive transfusion protocol.
The goal is to have the products ready to use in the case of the dynamic trauma patient.
The Thromboelastogram (TEG)Direct measures the four components of clot formation. When there is endolethial damage and bleeding, the sequence that your body takes to address it is as follows:
- Platelets migrate and form a plug
- Clotting factors aggregate and reinforce the platelets
- Fibrin arrives an acts like glue
- Other cells migrate and support the clot.
- Treated with platelets
- Treated with cryoprecipitate
- Treated with cryoprecipitate
- Treated with platelets
- Treated with an antifibrinolytics (tranexamic acid)
Red wine glass: a normal tracing with a normal reaction time and a normal amplitude. That patient just needs support and monitoring.
Champagne glass: a coagulopathic TEG tracing – thinned out, with less amplitude. This patient needs specific blood products.
Puffer fish or blob: a hyperfibrinolytic tracing. That patient will needs clot-stablizer.
TEG – like the FAST – can be repeated as the clinical picture changes.
The Trauma Death SpiralLethal triad of hypothermia, acidosis, and coagulopathy.
Keep the patient perfused and warm.
Each unit of PRBCs contains 3 g citrate, which binds ionized calcium, causing hypotension. In massive transfusion, give 20 mg/kg of calcium chloride, up to 2 g, over 15 minutes. Calcium chloride is preferred, as it is ionically readily available – just use a larger-bore IV and watch for infiltration. Calcium gluconate could be used, but it requires metabolism into a bioavailable source of calcium.
Prothrombin complex concentrate (PCC)Prothrombin complex concentrate (PCC) is derived from pooled human plasma and contains 25-30 times the concentration of clotting factors as FFP. Four-factor PCCs contain factors II, VII, IX and X, while 3-factor PCCs contain little or no factor VII.
The typical dose of PCC is 20-50 units/kg
In the severely hemorrhaging patient – you don’t have time to wait for the other blood products to thaw – PCC is a powder that is reconstituted instantly at the bedside.
Tranexamic acid (TXA)Tranexamic acid (TXA), is an anti-fibrinolytic agent that functions by stopping the activation of plasminogen to plasmin, and the degradation of fibrin. The Clinical Randomisation of an Antifibrinolytic in Significant Hemorrhage (CRASH-2) investigators revealed a significant decrease in death secondary to bleeding when TXA was administered early following trauma.
Based on the adult literature, one guideline is to give 15 mg/kg loading dose of TXA with a max 1 g over 10 minutes followed by 2 mg/kg/h for at least 8 h or until bleeding stops.
Resuscitative PearlsOur goal here is damage control. Apply pressure whenever possible. Otherwise, resuscitate, identify the bleeding source, and slow or stop the bleeding with blood products or surgery.
How Children are Different in TraumaIn adults, we speak of “permissive hypotension” (also called “balanced resuscitation” or “damage control resuscitation...

Diarrhea
Pediatric Emergency Playbook
07/01/20 • 50 min
Ask yourself -- again -- why is this not... appendicitis-torsion-intussusception-etc.
Admit sick children, but most go home, so...
Non-bloody, febrile -- no workup necessary; precautionary advice Non-bloody, afebrile -- be more skeptical, but generally same as above Bloody, febrile -- stool culture, follow up; do not treat empirically unless septic and admitted. Culture will dictate treat/no treat/how. Bloody, afebrile -- evaluate for hemolytic uremic syndrome, especially if under 5 years old: CBC, chemistries, UA, stool culture Evaluate Hydration StatusSelected References
Khan WA et al. Central Nervous System Manifestations of Childhood Shigellosis: Prevalence, Risk Factors, and Outcome. Pediatrics. 1999 Feb;103(2):E18
Lee JY et al. Diagnostic yield of stool culture and predictive factors for positive culture in patients with diarrheal illness. Medicine (Baltimore). 2017 Jul; 96(30): e7641.
Nelson JD et al. Treatment of Salmonella gastroenteritis with ampicillin, amoxicillin, or placebo. Pediatrics 1980; 65:1125.
Failure to Thrive
Pediatric Emergency Playbook
07/01/19 • 36 min
Failure to Thrive (FTT) is not just for the clinics. We need to be on the lookout, because if we find it, there is already a big problem.
Definitions of Failure to Thrive may quibble on the details, but for us in the ED:
- Consistently under 2nd percentile in weight over time
- "Falling off" the growth curve over 2 or more points
We can get around the longitudinal requirement by looking at weight as a "spot check" -- if grossly below weight without any other chronic condition, be alarmed.
Failure to thrive results from inadequate calories. This may be due to:
- Not enough offered
- Not enough taken
- Not enough absorbed
Any concern should trigger a more complete H&P (in audio).
Classic instructional video on the mother-infant dyad (scan through for various types).
After a focused H&P, you may need to admit the child for further workup, or to show that he can/cannot gain weight with routine care.
Remember, if you are the first one to bring this up, there is a real problem. By definition, an outpatient plan has failed. We will not be able to distinguish among the various possibilities of organic and non-organic causes (or mix thereof); our job is to be ready to catch it and act on it. The child's development, future intelligence, and welfare are at risk.
References
Birth to 24 months: Boys Weight-for-length percentiles and Head circumference-for-age percentiles
Birth to 24 months: Boys Length-for-age percentiles and Weight-for-age percentiles
Birth to 24 months: Girls Weight-for-length percentiles and Head circumference-for-age percentiles
Birth to 24 months: Girls Length-for-age percentiles and Weight-for-age percentiles
Jaffe AC. Failure to Thrive. Pediatrics in Review. 2011; 32(3)
Prutsky GJ et al. When Developmental Delay and Failure to Thrive Are Not Psychosocial. Hospital Pediatrics. 2016; (1):6
Mass Casualty Incident
Pediatric Emergency Playbook
06/01/19 • 32 min
No one ever wants to find himself in this situation. A factory explodes. A building catches fire. A multi-vehicle traffic collision. Or an act of terrorism.
Very quickly, we have to scrap business as usual. We have to adapt to our new circumstances.
Definition of a mass casualty incident (MCI):
An incident which produces multiple casualties such that emergency services, medical personnel and referral systems within the normal catchment area cannot provide adequate and timely response and care without unacceptable mortality and/or morbidity.
In other words, our demand far outpaces our resources.
"If you can hear the sound of my voice, follow me". Those patients are GREEN, minor.
Otherwise, we need a system to distinguish those who can be DELAYED, IMMEDIATE, or EXPECTANT (soon to be deceased).
Use Simple Triage and Rapid Treatment (START) for 8 or older, JumpSTART for less than 8 years of age.
An MCI drillFor Older Children, Adolescents, and Adults (8 or greater) -- START:
For Children less than 8 years of age (Infants Use Pediatric Assessment Triangle) -- JumpSTART:
- MCI Organizational Chart
Selected References
Briggs SM. Disaster management teams. Curr Opin Crit Care. 2005 Dec;11(6):585-
Culley JM, Svendsen E. A review of the literature on the validity of mass casualty triage systems with a focus on chemical exposures. American journal of disaster medicine. 2014; 9(2):137-150
FEMA IS 0100.b - Introduction to the Incident Command System (ICS), Student Manual. http://training.fema.gov/emiweb/is/is100b/student%20manual/02ics100b_sm_october2013.pdf. Accessed 03 MAY 2019.
Jensen J, Youngs G. Explaining implementation behaviour of the National Incident Management System (NIMS). Disasters. 2015 Apr;39(2):362-88. doi: 10.1111/disa.12103. Lee JS, Franc JM. Impact of a Two-step Emergency Department Triage Model with START, then CTAS, on Patient Flow During a Simulated Mass-casualty Incident. Prehosp Disaster Med. 2015 Jun 24:1-7.
Lerner EB, Schwartz RB, Coule PL, et al. "Mass Casualty Triage: An Evaluation of the Data and Development of a Proposed National Guideline." Disaster Medicine and Public Health Preparedness 2(Suppl. 1) 2008, pp S25-S34.

{kind=link}
From the Ashes of SIRS: The Phoenix Sepsis Score
Pediatric Emergency Playbook
06/01/24 • 23 min
pemplaybook.org
Show more best episodes

Show more best episodes
FAQ
How many episodes does Pediatric Emergency Playbook have?
Pediatric Emergency Playbook currently has 103 episodes available.
What topics does Pediatric Emergency Playbook cover?
The podcast is about Health & Fitness, Ems, Pediatrics, Medicine, Podcast, Podcasts, Education and Foam.
What is the most popular episode on Pediatric Emergency Playbook?
The episode title 'DKA Like A Boss' is the most popular.
What is the average episode length on Pediatric Emergency Playbook?
The average episode length on Pediatric Emergency Playbook is 34 minutes.
How often are episodes of Pediatric Emergency Playbook released?
Episodes of Pediatric Emergency Playbook are typically released every 30 days, 23 hours.
When was the first episode of Pediatric Emergency Playbook?
The first episode of Pediatric Emergency Playbook was released on Sep 1, 2015.
Show more FAQ
Show more FAQ